Uterine Fibroids Management
The treatment of uterine fibroids depends on its size and location, the patient’s age, symptoms, desire to maintain fertility, and access to treatment.
The ideal treatment should satisfy four goals:
-
relief of signs and symptoms,
-
sustained reduction of the size of fibroids,
-
maintenance of fertility (if desired),
-
avoidance of harm.
The first classification that establishes the path of the patients with uterine fibroids is their subdivision in Symptomatic and Asymptomatic women.
Asymptomatic women
About half of women with uterine fibroids are asymptomatic. It means their clinical condition don’t affect their life.
Probably these women don’t even know to have a fibroid or have discovered it during a random gynecological visit or because they are trying to achieve pregnancy.
Since there is minimal concern for malignancy in women with asymptomatic fibroids, clinical surveillance is preferred for management.
Actually, most of them have some symptoms such as abundant bleeding that over time can give fatigue or anemia. Moreover, data show that the average growth rate for uterine fibroid was found to be 9% over 6 months.
For these reasons clinical surveillance isn’t free of consequences.

Symptomatic women
In women with symptomatic uterine fibroids the treatment must take in consideration if the patient wishes to preserve fertility.
In order to preserve fertility or uterus, all the medical options aim to reduce symptoms (especially heavy bleeding) since most of them have not effects on fibroid.
For what concern women in post-menopause or do not want to preserve the uterus or when fibroid size strongly affects the quality of life, surgery represents the only option.

Medical treatments
Medical approach to uterine fibroid can have different aims.
Bleeding reduction
The choice must to be tailored to the patient symptomatology and with her life-project, contraceptive or creative.
Hormonal contraceptives are the most common options when there isn’t a wish of pregnancy.
This approach has the aim to reduce menstrual bleeding stopping the ovulatory cycle.
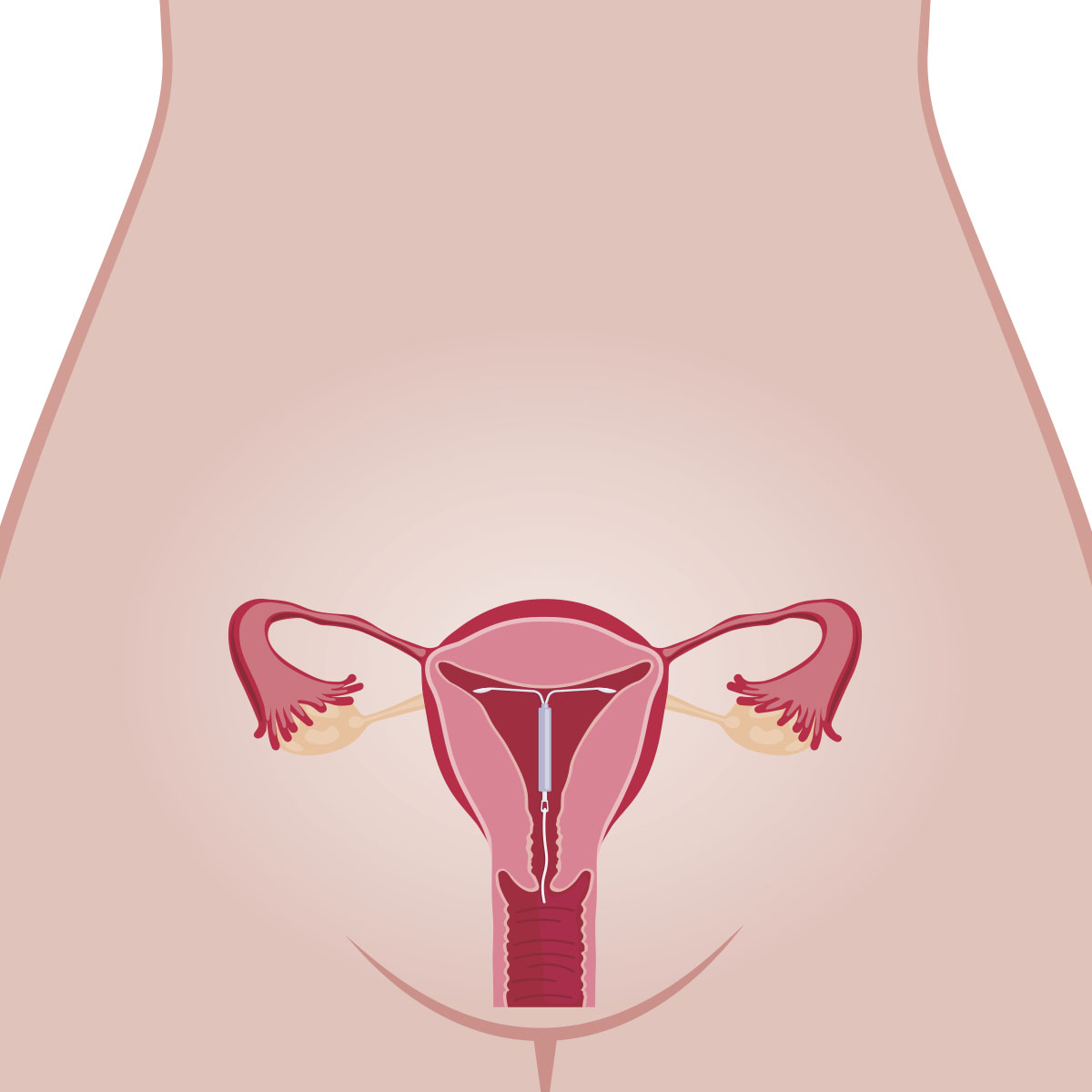
The levonorgestrel IUD (intrauterine releasing system) is the first approach due to its greater reduction in menstrual blood loss vs. oral contraceptives.
Tranexamic acid is an oral nonhormonal antifibrinolytic agent that significantly reduces menstrual blood loss compared with placebo.
Gonadotropin releasing hormone (GnRH) agonists are options for patients who need temporary relief from symptoms preoperatively or who are approaching menopause.
GnRH agonist putting women into a temporary postmenopausal state indeed the main side effects are similar to menopausal syndrome: hot flashes, vaginitis, sweating, and change in breast size.
This affects the long-term use of these agents.
Ulipristal is an SPRM (selective progesterone receptor modulators) approved as a contraceptive in the United States showing to reduce mean blood loss, decrease fibroid volume by more than 25%, and induces amenorrhea in significantly more patients.
FDA, due to its side effects on liver, didn’t approve the its use for the fibroid management.
In other countries, it is used as a preoperative treatment of fibroids in adult women who are eligible for surgery.
Treatment is limited to three months of continuous use.
Pain Relief
Nonsteroidal Anti-inflammatory Drugs are the primary choice to improve pain.
These agents can reduce blood loss but are less effective then hormonal treatment.
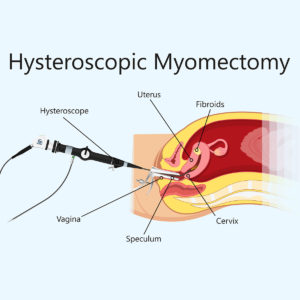
Surgery
Myolysis
Myolysis is a minimally invasive procedure targeting the destruction of fibroids via a focused energy delivery system such as heat, laser, magnetic resonance.
This less-invasive procedure is well tolerated, although risks include localized pain and heavy bleeding.
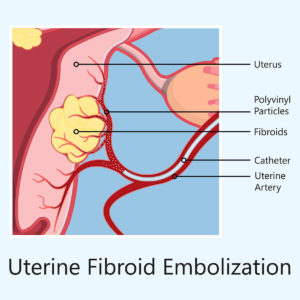
Uterine Artery Embolization
Uterine artery embolization is an option for women who wish to preserve their uterus or avoid surgery because of medical comorbidities or personal preference.
It is an interventional radiologic procedure in which occluding agents are injected into one or both of the uterine arteries, limiting blood supply to the uterus and fibroids.
The most common complication is postembolization syndrome, which is characterized by mild fever and pain, and vaginal expulsion of fibroids.
There is insufficient evidence on the effect of uterine artery embolization on future fertility.
Hysterectomy
Hysterectomy is the last-resort treatment for uterine management. It consists a definitive removal of uterus so it is a feasible option only for women with symptomatic fibroids who do not wish to preserve fertility.
New alternative agents
Epigallocatechin gallate
Epigallocatechin gallate is the major catechin in green tea, a natural product, commonly used by women for multiple purposes.
Epigallocatechin gallate (EGCG) exhibits several biological effects, including anti-inflammatory, antiproliferative, and antioxidant effects.
The effectiveness of epigallocatechin gallate has been studied on fibroid biology. Experimental results showed that epigallocatechin gallate inhibits the proliferation of human leiomyoma cells.
Interestingly, epigallocatechin gallate dramatically reduced the volume and weight of fibroids in both animal and human trials.
These data suggest a promising alternative in which the burden of this disease could be reduced by making green tea extract available to women who have uterine fibroids.
EGCG might be particularly useful for long term use in women with low fibroid burden to arrest its progression and avoid the development of severe symptoms needing major surgery.

Vitamin D
Hypovitaminosis D has been recently associated with a higher prevalence of uterine fibroids.
Furthermore, some authors reported that vitamin D serum levels are inversely correlated with the severity of uterine fibroids.
Vitamin D is known for its antiproliferative and immunomodulatory hormone with a well-established role in the maintenance of calcium homeostasis.
Moreover, vitamin D inhibits the growth and promotes the apoptosis of fibroid cells in “in vitro” studies, and it seems to reduce the fibroid size in “in vivo” animal models.
According to these findings, vitamin D supplementation might be an effective, safe, and low– cost therapy in the primary prevention and treatment of uterine fibroids.
The plausible stabilizing effect of vitamin D supplementation on size and number of “small burden” uterine fibroids could be most beneficial, especially in pre and perimenopausal women. The aim of the Vitamin D supplementation would be to prevent the possible growth of fibroids and the onset of fibroid-related symptoms, as well as to reduce the need for surgery or conventional medical therapy.
- Maria Syl D. et al. Am Fam Physician. 2017 Jan 15;95(2):100-107
- Islam MS. et al. J Clin Endocrinol Metab. 2013 Mar;98(3):921-34.
- Zhang D. et al. Fertil Steril. 2010 October ; 94(5): 1887–1893
- Roshdy E et al. Int J Womens Health. 2013 Aug 7;5:477-86
- Sabry M. et al. Int J Womens Health. 2013;5:93-100
- Blauer M. et. Fertil Steril. 2010 Oct;94(5):1887-93
- Ciavattini A. et al. Medicine (Baltimore). 2016 Dec;95(52):e569